Etiquetado: Tosferina
Tos ferina, brotes y mortalidad | ¿De quién es la responsabilidad?

Traducción automatizada de la versión original Kinkhoest, uitbraken en sterfte | Wiens verantwoordelijkheid? con autorización del autor
En las últimas semanas se ha producido un notable aumento del número de infecciones de tos ferina detectadas. NOS Journaal lo achaca al descenso de la cobertura vacunal, apoyado, por supuesto, por la brigada de vacunación de los profesionales de Groningen y Rotterdam.
Mi colega español Juan Gérvas, antiguo médico generalista y ex profesor de la Escuela de Salud Pública de la Universidad Johns Hopkins, escribió un interesante artículo al respecto. Arroja una luz diferente sobre estos asuntos de la que nos quieren hacer creer los médicos, funcionarios y políticos de los Países Bajos, que están en conflicto de intereses. He escrito una reflexión al respecto.
Vacuna subóptima
La vacuna contra la tos ferina es necesaria, pero necesita mejoras urgentes. En el contexto de los brotes y muertes por tos ferina, es importante darse cuenta de que el problema no es el movimiento antivacunas, sino la propia vacuna. La vacuna contra la tos ferina es poco eficaz. Necesitamos una vacuna mejor, que genere inmunidad duradera y evite la infección y la transmisión.
Así pues, tenemos una vacuna contra la tosferina que tenemos que reconocer que funciona mal. Por esta razón, actualmente tenemos que vacunar y revacunar varias veces. La industria se beneficia enormemente de ello.
Es una vergüenza que se haya abandonado la mejora de la vacuna cuando durante décadas en las que se han acumulado pruebas empíricas de su ineficacia. Más vergonzosa aún es la solución fácil de vacunar a las embarazadas. Es una vergüenza que el feminismo tolere esta transformación de la mujer embarazada en un útero. Y es una vergüenza que los ministerios de Sanidad estén dirigidos por la industria y nunca hayan exigido mejores vacunas contra la tosferina.
Además, no existe una forma comercial separada de administración de la vacuna, por lo que hay que revacunar a la embarazada contra la tosferina, el tétanos y la difteria al mismo tiempo (en España – editorial). Una y otra vez, dos vacunas «añadidas» innecesarias. Además, la ineficacia de la vacuna obliga a las bacterias a evolucionar hacia formas más agresivas. La ética y la deontología médicas están en caída libre.
Los responsables de la actual epidemia de tosferina, con muertes incluidas, son las autoridades sanitarias encabezadas por el Ministerio de Sanidad, las industrias y las asociaciones ‘científicas’ (de salud pública, epidemiología, economía de la salud, médicos de cabecera, medicina general, pediatría, etcétera).
Reseña
Juan Gérvas pone el dedo en la llaga. La vacuna contra la tos ferina no es suficientemente buena. Es uno de los principales factores de infecciones y muertes. Sin embargo, en nuestro país, investigadores con conflictos de intereses, profesionales de Groningen y políticos ignorantes aprovechan la epidemia de tos ferina para culpar a los «antivaxxers», lo cual es completamente falso.
Los representantes más destacados de la industria de las vacunas en los Países Bajos desde hace décadas proceden de los círculos D66. Debe haber una compulsión a la vacunación, claman. Sus partidarios, casi más que los del VVD, creen en el efecto beneficioso de la industria para la salud de las personas. Con ello, este partido va diametralmente en contra de sus propios principios de autodeterminación y ética médica.
D66 no tiene ningún conocimiento sustantivo de la ciencia médica, como vimos durante la pandemia de coronavirus. La vacuna contra el coronavirus fue un trágico fracaso y la vacuna contra la tos ferina necesita mejoras urgentes. Y la vacuna de la gripe no funciona. Este partido no dice nada al respecto.
Dar la vuelta a las cosas y afirmar lo contrario es un mecanismo cotidiano, pero también desenfrenado en la política de los neoliberales. Me he referido a ello muchas veces. Freud lo describió en Psicopatología de la vida cotidiana. Siempre es más fácil culpar a la gente que sabe pensar.
La política gubernamental de los últimos años durante la pandemia condujo exactamente a lo contrario de lo que pretendía. Los ciudadanos ya no creen al gobierno. Y esto se debe principalmente a los asesores con intereses contrapuestos que, con una arrogancia sin precedentes y descarada, afirmaron cosas sobre las vacunas del coronavirus que no eran ciertas. Si estos mismos asesores y el gobierno piensan que la gente lo ha olvidado, se equivocan. El gobierno y sus asesores son los principales culpables de la caída de las tasas de vacunación, y eso es lo que hay que abordar.
Visto así, cabe preguntarse cómo va a abordar el Gobierno este problema. Me temo lo peor. La vacuna contra la tos ferina es menos eficaz desde 1996, pero el gobierno no se responsabiliza de ello en modo alguno. Al mismo tiempo, el RIVM informa en su página web de que si un niño tiene tosferina y se encuentra bien puede ir sin más a la guardería o al colegio. Un adulto con tosferina también puede simplemente ir a trabajar. Lo único que está haciendo el Gobierno es intensificar aún más la polarización. Este gobierno nos está llevando «de Guatemala a Guatepeor».
El NOS News haría bien en dejar de inmiscuirse en cuestiones médicas y especialmente en los tratamientos farmacológicos. Es ir demasiado lejos y nadie se enterará, excepto la industria farmacéutica y los neoliberales. NOs, entreviste también a expertos independientes para variar.
Pertussis (outbreaks and deaths). It’s not the anti-vax, it’s the vax.
Juan Gérvas, Retired Rural General Practitioner, CESCA Team, Madrid, Spain
jjgervas@gmail.com http://www.equipocesca.org @JuanGrvas
Mercedes Pérez-Fernández, Internal Medicine Specialist, Retired General Practitioner, CESCA Team, Madrid, Spain. mpf1945@gmail.com
Summary
Pertussis vaccine is a necessary one, but it needs urgent improvement. In the face of pertussis outbreaks, and pertussis deaths, it is important to realise that the problem is not the anti-vaccine movement but the vaccine. The pertussis vaccine is of low effectiveness. We need a better vaccine (one that generates lasting immunity and prevents infection and transmission).
Introduction
The scandal in many countries over the whooping cough death of a baby whose mother had not been vaccinated at the end of her pregnancy it is a common fact. See for example: “Jerusalem baby dies of whooping cough, mother not vaccinated”
The headline is biased and copied in all the media (print and online press, radio, television, etc.), as it incites the blame on the pregnant woman, and has managed to create a real popular lynch mob, including the accusation of murder. No one has asked why pregnant women should be vaccinated, nor why a public health problem has become a personal problem.
It is convenient to bring out the news now because there is a whooping cough epidemic, so that the population revolts against the «anti-vaccine» and not against those who maintain and promote an inefficient vaccine: the health authorities (the Ministry of Health and others), the industries and the «scientific» societies (public health, epidemiology, health economics, family/general medicine,
paediatrics, etc.).
It should also be noted that the pertussis vaccine does not exist as such, but is part of a triple bacterial vaccine (pertussis, tetanus and diphtheria)
Whooping cough vaccine is highly ineffective The pertussis vaccine was first used successfully in 1929. Given its significant local reactogenitic capacity and other frequent adverse effects (in addition to the usual local inflammatory effects and fever associated with many vaccines, whole-cell pertussis vaccines sometimes trigger prolonged crying and febrile convulsions and, very rarely, hypotonic–hyporesponsive episodes), which led to rejection, a «light» version was prepared (acellular, with less antigenic capacity and less capacity to stop contagion but fewer adverse effects) which was introduced into practice from the end of the 1980/90s (first in Japan, 1981, later in many countries, for example in 1998 in Spain, full implementation in 2005).
We currently use a combined vaccine, diphtheria, tetanus, acellular pertussis, DTaP, with a high load (in childhood), and dTpa, also Tdap, diphtheria-tetanus-acellular pertussis vaccines with a low load, with a lower amount of diphtheria and pertussis (in adolescents and adults).
Pertussis vaccine is a necessary vaccine but needs urgent and profound improvement. It fails with incomplete vaccination but even with correct vaccination.
For example, one study in California (the USA) found that protection against pertussis waned during the 5 years after the fifth dose of DtaP. In Alberta, Canada, of the 81.6% (n = 1,348) pertussis cases with immunization records, 48.3% were up-to-date with immunization. The pertussis cases that were up-to-date with their immunization were older (median age 12.9 years) as compared to those with incomplete (median age 9.7 years) or no pertussis immunization (median age 3.8 years).
In one study of an outbreak in Alicante (Spain) with 104 reported cases of pertussis confirmed by PCR, 85 cases (82%) had correctly complied with the 5-dose vaccine schedule. The protection time was 2.1 years with Tdpa and 5.1 years with DTaP. In other words, most cases occur in correctly vaccinated patients, and protection lasts at most 5 years: In Ontario, Canada, the conclusion was: “We identified good early vaccine effectiveness, which rapidly declined when time since last vaccination surpassed 4 years, in a population with relatively stable disease incidence”
In Spain, all vaccinations are free of charge, and are widely accepted by the population. But sometimes vaccines fail. For example, revaccination of pregnant women is not enough to prevent deaths from whooping cough: «A baby dies in Castellón from whooping cough (the mother was vaccinated)». «A baby dies of whooping cough in Jaén despite the fact that her mother had been vaccinated during pregnancy».
Whooping cough outbreaks after the «honeymoon».
If immunity wanes at five years, and acellular vaccination was completed in 2005 in Spain, a resurgence of the disease is to be expected in Spain from 2010 onwards. And so it is, according to data recorded by the Institute of Health Carlos III (page 8, table 1) which show that the incidence increased more than 7-fold between 2011-19 compared to 2005-10.

INFORME EPIDEMIOLÓGICO SOBRE LA SITUACIÓN DE LA TOSFERINA EN ESPAÑA, 2023
As noted above, these outbreaks mainly affect patients who have been correctly vaccinated.
The public health response is to maintain such a useless pertussis vaccine (not to improve it), to increase the number of revaccinations and to use women as a womb (vaccinating them with a triple vaccine that adds two unnecessary re-vaccinations).
Problems with the pertussis vaccine
The pertussis vaccine has several problems, such as a) its short duration of immunity (between 1 and 5 years), b) its impact on the bacterium itself (bordetella), forcing its evolution into more aggressive strains that evade vaccine immunity, and c) its ineffectiveness on mucous membranes, so prevents neither contagion nor transmission of the bacterium (and therefore does not create herd immunity).
Within years of childhood vaccination, pertussis emerges in adolescents and young adults, who pass it on to their mothers and infants.
We have been studying the pertussis bacterium, the disease and the vaccine for over a hundred years, yet:
1/ the mechanisms of human immunity to pertussis are not fully understood
2/ there is no satisfactory vaccine
3/ there is no sensible and useful explanation for the outbreaks that occur in well-vaccinated populations in developed countries.
«Toward a new vaccine for pertussis».
«Coping Strategies for Pertussis Resurgence».
Questions and answers
1.- Was pertussis vaccine not ineffective before and is it ineffective now?
The pertussis vaccine has always been of low effectiveness, but even more so when switching to «acellular» (to avoid the rejection of parents and infants due to the intense local reactions of the cellular, «complete» vaccine). The pertussis vaccine is a necessary vaccine, but it has always been in need of profound and urgent improvement.
2.- If it was not before, what has changed?
It has changed because the «honeymoon» period has ended and immunity has faded, which means that a large part of the population is now «infectable» by the bacterium. This honeymoon is not maintained because the vaccine does not prevent the disease but hinders the usual spontaneous re-immunisation of the population (passing the disease does not create lasting immunity, but successive infections maintain it throughout life).
3.- Does whooping cough kill?
Whooping cough is a mild disease (very annoying because of persistent cough) in affluent countries where adequate clinical care is provided, but whooping cough is serious and causes death when it is associated with inequity, poverty, hunger and poor living conditions and where there is a lack of a public health system with universal coverage.
«The World Health Organization estimates that in 2018 there were about 16 million cases and 195,000 deaths from whooping cough worldwide, but more than 95 per cent were in developing countries«.
It is worth bearing in mind that pertussis can kill especially young children under the age of one year and especially those under two months, who have no antibodies left from their mother, have not yet been vaccinated and have an immature immune system to defend themselves against infection.
4.- If this has always been the case, what is the point of repeated administration in childhood and pregnancy?
In Spain, vaccination of pregnant women is recommended «from the 27th week of pregnancy, but preferably in week 27 or 28′′. Subsequently, the baby receives two doses, at 2 and 4 months of life, a first booster dose at 11 months and another at 6 years of age. In some Autonomous Communities, a fifth dose is added in adolescence.
As a lesser evil, so much revaccination does make sense (we have a lousy vaccine, it must be acknowledged, we have to revaccinate and revaccinate to remedy it, even if it means big business for the industry).
But it is a shame to give up on demanding vaccine improvement after decades of empirical proof of its inefficiency. Even more shameful is the easy solution, and forever, of vaccinating pregnant women (and with triple presentation!).
It is a disgrace that feminism tolerates this transformation of the pregnant female in a woman’s womb.
And it is a disgrace that public health is run by industry and never demands better vaccines against whooping cough.
Moreover, there is no separate commercial presentation of the vaccine, so that the pregnant woman has to be revaccinated at the same time against whooping cough, tetanus and diphtheria. Again and again two unnecessary «added» vaccines. Moreover, the vaccine is forcing the bacteria to evolve into more aggressive forms.
Medical ethics and deontology are in free fall.
Summary
The cause of the cause of the current pertussis epidemic, with its deaths, is the responsibility of the health authorities (led by the Ministry of Health), the industries and the «scientific» societies (public health, epidemiology, health economics, family/general medicine, paediatrics, etc.).
“Tosferina. Brotes y muertes. No son los antivacunas, es la vacuna. spanish version
“Tosferina. Epidemias sin antivacunas y la mujer como vientre”
Tosferina (brotes y muertes). No son los antivacunas, es la vacuna
Juan Gérvas, médico general rural jubilado, Equipo CESCA, Madrid, España. jjgervas@gmail.com www.equipocesca.org @JuanGrvas
Mercedes Pérez-Fernández, Especialista en Medicina Interna, médico general jubilada, Equipo CESCA, Madrid, España. mpf1945@gmail.com
Resumen: La vacuna de la tosferina es una vacuna necesaria, pero que precisa mejora profunda y urgente. Ante los brotes de tosferina, y las muertes por tosferina, es importante tener en cuenta que el problema no son los antivacunas sino la vacuna. La vacuna de la tosferina es una vacuna ineficiente. Precisamos una mejor vacuna (que genere inmunidad perdurable y que evite el contagio y la transmisión).
Introducción
El escándalo actual en España (finales de marzo de 2014) ante la muerte por tosferina de un bebé cuya madre no se había vacunado al final de la gestación es artificial ya que la muerte del bebé fue el año pasado
El titular es además tendencioso, copiado en todos los medios (prensa en papel y virtual, radios, televisiones, etc.), pues incita a cargar la culpa en la mujer gestante, y ha conseguido crear un verdadero linchamiento popular, incluyendo la acusación de asesinato. Nadie se ha preguntado por qué hay que vacunar a la embarazada, ni porqué un problema de salud pública acaba convertido en un problema personal.
Conviene sacar ahora la noticia porque hay epidemia de tosferina, para que la población se revuelva contra los «anti-vacunas» y no contra quienes mantienen y promueven una vacuna ineficiente y muy mejorable: las autoridades sanitarias (el Ministerio de Sanidad a la cabeza), las industrias y las sociedades «científicas» (de salud pública SESPAS, epidemiología SEE, economía de la salud AES, etc.).
Conviene señalar, también, que la vacuna de la tosferina no existe como tal, está integrada en una triple bacteriana (tosferina, tétanos y difteria).
La vacuna de la tosferina es muy ineficiente
La vacuna de la tosferina se empleó por primera vez con éxito en 1929. Dada su importante capacidad reactógena local (y otros efectos adversos frecuentes, como convulsiones febriles, lloro persistente, e infrecuentes como episodios de hipotonía), que llevaba al rechazo, se preparó un versión “ligera” (acelular, con menor capacidad antigénica y de frenar contagios pero menos efectos adversos) que se introdujo en la práctica desde finales de los 80 del pasado siglo (en 1998 en España, implantación completa en 2005)

En la actualidad empleamos una vacuna combinada, difteria, tétanos, tosferina acelular, DTPa, de carga elevada en la infancia, y dTpa, también Tdap, vacunas difteria-tétanos-tosferina acelular de carga baja, con menor cantidad de difteria y tosferina, en adolescentes y adultos.
La vacuna de la tosferina es una vacuna necesaria, pero que precisa mejora profunda y urgente. Falla con la vacunación incompleta pero incluso con vacunación correcta.
Por ejemplo, este estudio de un brote en Alicante en que notificaron 104 casos de tosferina confirmados por la PCR y 85 casos (82%) se habían cumplido correctamente el calendario de 5 dosis de la vacuna. El tiempo de protección fue de 2,1 años con la dTpa y de 5,1 con la DTPa. O sea, la mayoría de los casos se dan en pacientes correctamente vacunados, y la protección dura como mucho 5 años. En los niños y adolescentes bien vacunados y revacunados, la eficacia es muy baja. Por ejemplo, siendo necesaria la revacunación de la embarazada ello no es condición suficiente para evitar muertes y se publicaron casos tambien como noticia periodística, en 2016 en Castellón y Jaén
Brotes de tosferina tras la “luna de miel”
Si la inmunidad se desvanece a los cinco años, y se terminó de introducir la vacuna acelular en 2005, es de esperar en España el resurgir de la enfermedad a partir de 2010. Y así es, según los datos registrados por el Instituto de Salud Carlos III (pagina 8, tabla 1) que demuestran que la incidencia se multiplica por más de 7 entre 2011-19 respecto a 2005-10

Como hemos señalado, dichos brotes afectan, fundamentalmente, a pacientes correctamente vacunados. La respuesta de salud pública es mantener la, tan inútil vacuna tosferina, no mejorarla, incrementar el número de revacunaciones y utilizar a la mujer como vientre (vacunándola con una triple vacuna que añade dos vacunas innecesarias).
Problemas de la vacuna de la tosferina
La vacuna de la tosferina presenta problemas varios, como:
1/ baja duración de su inmunidad (entre 1 y 5 años).
2/ impacto sobre la propia bacteria (bordetella) forzando su evolución a cepas más agresivas que evaden la inmunidad vacunal.
3/ su ineficacia sobre mucosas por lo que no evita ni el contagio ni la transmisión de la bacteria (y por tanto no crea inmunidad de grupo).
Al cabo de los años de la vacunación en la infancia, la tosferina emerge en adolescentes y jóvenes, que la contagian a sus madres y a los bebés.
Llevamos más de cien años estudiando la bacteria de la tosferina, la enfermedad y la vacuna y sin embargo a/ no se conocen a fondo los mecanismos de la inmunidad humana a la tosferina, b/ no existe una vacuna satisfactoria y c/ no hay una explicación sensata y útil para los brotes que se producen en poblaciones bien vacunadas en los países desarrollados
Preguntas y respuestas
1.- ¿La vacuna de la tosferina antes no era ineficiente y ahora sí?
La vacuna de la tosferina ha sido siempre ineficiente pero más al cambiar a «acelular» (para evitar el rechazo de padres e infantes por las intensas reacciones locales de la vacuna celular, “completa”). La vacuna de la tosferina es una vacuna necesaria, pero que de siempre ha precisado mejora profunda y urgente.
2.- Si antes no lo era, ¿Qué ha cambiado?
Ha cambiado porque se ha acabado el periodo de «luna de miel» y se ha desvanecido la inmunidad lo que hace que gran parte de la población sea ahora «infectable» por la bacteria. Dicha luna de miel no se mantiene porque la vacuna no impide la enfermedad, pero además dificulta la habitual re-inmunización espontánea de la población (pasar la enfermedad no crea inmunidad duradera, pero los sucesivos contagios van manteniéndola a lo largo de la vida).
3.-La tosferina ¿mata?
La tosferina es enfermedad leve (muy molesta por la tos persistente y quintosa) en los países enriquecidos, donde se presta atención clínica adecuada, pero la tosferina es grave y causa de muerte cuando se asocia a inequidad, pobreza, hambre y malas condiciones de vida y donde falta de un sistema sanitario público de cobertura universal:
Conviene tener en cuenta que la tosferina puede matar especialmente a los niños pequeños menores de un año y, sobre todo, a los menores de dos meses, en los que ya no quedan anticuerpos (defensas) que le pasó la madre, todavía no han sido vacunados y tienen un inmaduro sistema inmunitario para defenderse de la infección.
4.-Si siempre lo ha sido ¿Qué sentido tiene su administración repetida en la infancia y en el embarazo?
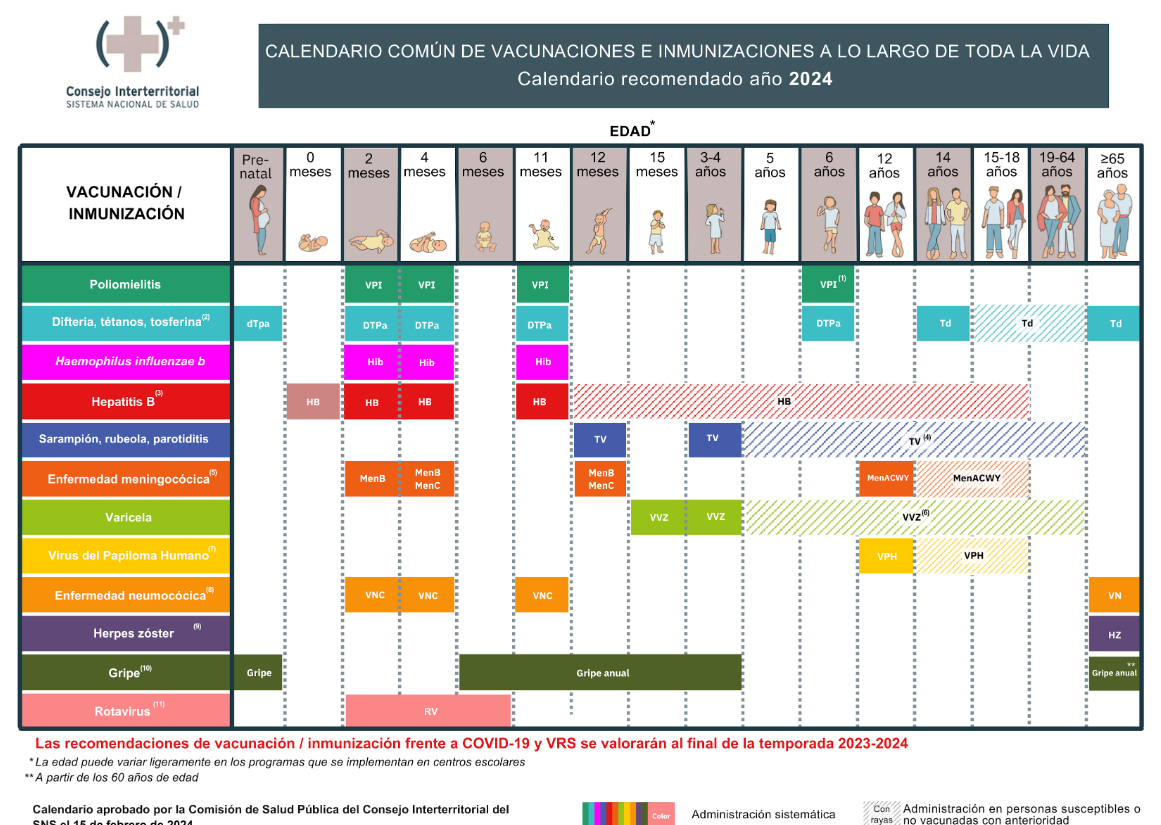
En España se recomienda la vacunación de la embarazada “a partir de la semana 27 de embarazo, pero preferiblemente en la semana 27 o 28″. Posteriormente, el bebé recibe dos dosis, a los 2 y 4 meses de vida, una primera dosis de recuerdo a los 11 meses y otra a los 6 años. En algunas Comunidades Autónomas se añade una quinta dosis, en la adolescencia.
Como mal menor, sí tiene sentido tanta revacunación (tenemos una pésima vacuna, es obligado reconocerlo, hay que revacunar y revacunar para remediarlo por más que ello sea gran negocio para la industria y gran fuerza para «la salud pública»).
Pero es una vergüenza renunciar a exigir la mejora de la vacuna después de décadas de comprobación empírica de su ineficiencia. Es una vergüenza todavía mayor la fácil solución, y para siempre, de vacunar a la mujer embarazada(¡y con triple presentación!). Es una vergüenza que el feminismo tolere esta cosificación como vientre de la mujer. Y es una vergüenza que la salud pública esté manejada por la industria y no exija nunca mejores vacunas contra la tosferina.
Además, no hay presentación comercial aislada de la vacuna por lo que la gestante se tiene que revacunar, al tiempo contra tosferina, tétanos y difteria. Una y otra vez dos vacunas “añadidas” innecesarias. Además, la vacuna está forzando la evolución de la bacteria, a formas más agresivas. La ética y la deontología médica, en caída libre.
Síntesis
La causa de la causa de la actual epidemia, con sus muertos, es responsabilidad de las autoridades sanitarias (con el Ministerio de Sanidad a la cabeza), las industrias y las sociedades «científicas» (de salud pública SESPAS, epidemiología SEE, economía de la salud AES, etc.)
“Tosferina. Epidemias sin antivacunas. Y la mujer como vientre”
