Do it right
Do it right, do the best or do it better?.
by Angel Ruiz Tellez @artcymap
Marshall and Warren suffered fierce criticism for 20 years from much of the medical profession, who first ridiculed their questions and then their findings.
What was to “do things right?”. Clearly, to have peace of mind, reduce work and life stress, 8 hours of sleep, no spicy foods, giving up antacids, pyloroplasty, and vagotomy in stubborn cases.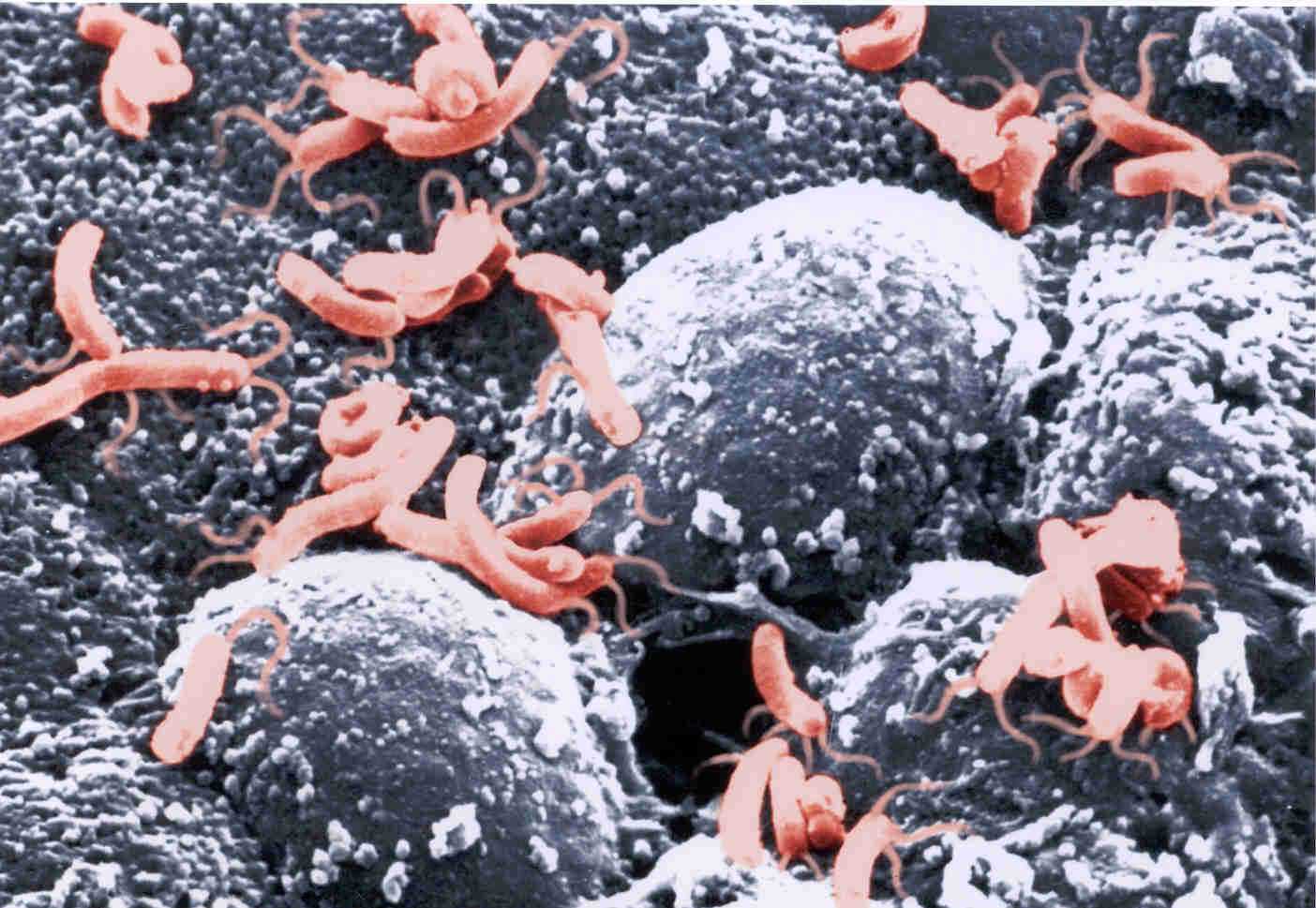
How could it be possible that the stomach and duodenum’s ulcers were infectious? Both doubted the dogmas and the clear ideas that were prevailing, away from the ‘security’ of the “evidence of the moment“. They even inoculated the bacteria to themselves to prove their findings. Twenty-three years after their findings in 1982, they received the Nobel Prize for the discovery and proof of the infectious involvement of Helicobacter Pylori, in the genesis of peptic pathology.
 Now that we know more, can all stomach pains be susceptible of being considered ulcerative pathology? Does the presence of h. pylori in a gastric cultivation of an asymptomatic patient confirm the necessity of eradicating therapy? What does the algorithm tell us? What does experience tell us?
Now that we know more, can all stomach pains be susceptible of being considered ulcerative pathology? Does the presence of h. pylori in a gastric cultivation of an asymptomatic patient confirm the necessity of eradicating therapy? What does the algorithm tell us? What does experience tell us?
What is experience? Today we begin to understand this. It is the ‘efferent copy’ which is created and launched by the brain . It is the anticipated copy of the immediate effects that will be produced, which our brain sends to our muscles and senses. It is the one that allows me to drive without paying attention. Were you not surprised, even startled occasionaly, realizing that you have driven 100 miles talking on the phone; or daydreaming without having even realized it? This ‘efferent copy‘ only wakes up the automatic pilot when it meets something different from the known and expected.
The doctor, before seeing each patient and after many years of practice, consciously and basically unconsciously, has created ‘efferent copies‘ of the condition of normality and pathology status. This huge set of information received and recorded in the brain is not a simple computer diagnostic code, which is today´s intention to ‘launch’ a therapeutic behaviour through a simplistic algorithm on an electronic health record.
The algorithm and the clinical guide, should only be oneof those stimuli and perceptions that the brain balances for the clinical act, along with the hundreds of information unconsciously recorded on the acquisition of ‘clinical experience’. And it should never be reduced to onlyone, which is what they are trying to impose, for simple economic reasons disguised as scientism; imposing at the time of prescription or indication of a diagnostic or therapeutic intervention, an algorithm that requires explicitly, or by exhaustion (e.g. written justifications for the election, 20 or more mouse clicks, more or less veiled threats…etc) to do something that is centered in the ‘evidence of the moment ‘.
There is no computer system that has even recorded 1% of the reality of this clinical complexity.
The way to be seated in the waiting room, the presence or type of companion, the dress code, the expression, if you wait sitting or wandering around, the way into the consultation room, its look, its colour, its odour, its dissociated corporal-oral expression, the movement of his hands, the way they greet you, the way they sit.…etc. There is lots of information that the brain has captured in fragments, in glimpses when the door of the consultation opens from one patient to another, and that nevertheless, they have been creating a huge database of information and knowledge, unconscious and intuitive, a substratum of clinical excellence and expertise.
Has anyone seen Dr. House clicking on a damn computer when developing a diagnostic?
Expert thinking is hypothetical and intuitive and never algorithmic as it is intended to be imposed with a simple and limited algorithm of spending, wrongly called diagnostic, by these new econo-scientists methods that the directive’s ignorance has imposed as a last resort.
A month ago, a colleague from a Valencian medical directive team, told me that she was delaying the order to remove the < ESC > option that allowed the professional to skip the fateful “brainwash tunnel” of therapeutic indication algorithm. This was because some doctors (which she considered to be sensible and competent) told her that the simplicity of it limited the access to some indications or other tests, for the cases in which ‘something’, where their intuition (‘efferent copy’) forced them to indicate it, despite what the algorithm had told them.
It is very important to be aware of the selection of “Model of skyline’s performance’s type” that rules the Health Organization. There are three possible scenarios, with very different consequences: «do it right«, «do the best» or «do it better».
Do it right is the scenario chosen in the commented examples of algorithms or protocols above.
A group of professionals, with different views and interests and unique influences, ended agreeing with respect to probabilistic values of central tendency or average value, a procedure with the aim of general orientation. These, that are the clinical guidelines, we, the professionals, are deeply grateful for, but once read we put them in the storage of information and experience. Up to here everything is a plus.
When a non-clinical professional, without ‘efferent copy ‘, in general, Directors, Pharmaceutical Directors, non-pharmacologist, without any clinical experience or financial responsibility, see this Guide, lacking the ‘efferent copy’ that allows them to recognize reality, they believe they have discovered, in their daring ignorance, the tool of professional pressure that will end up with costs, without having to fall into the arena of Behavioural Management when the system is unable to discern between those who spend very little, those who close the door, those who are highly efficient, or in between those who spend a lot and those who work hard and spend or those who are wasters (Diagram X ).
That organization will have converted the means of support, the algorithm, on a final purpose. The professional can only “do it right” if he complies with the algorithm. The consequence is serious. The organization leans to the procedural mentality, to bureaucracy, to disaffection with the patient that is ‘out’ of the norm, to thoughtlessness and to mediocrity. All our efforts of improvement will be reduced to a few “quality” groups, whose unique and sublime mission will be reading the anglo-saxon bibliography to ‘update’ the current procedure, with the new third party revisions i.e. those who hesitate, think, evaluate, prove, make mistakes, conclude and publish several years later – our manna from heaven. Meanwhile we will have lost time and we focused the entire organization to abide by the previous algorithm protocol installed in the measurements of Portfolio of Services. How were the non “modern and up–to–date” considered, those who did not believe in cardiovascular prevention of hormone replacement therapy! How damaged were and are (in measurements of Service portfolios) those intuitive professionals able to solve without having to fill out the mediocre procedure!
 Even worse than the above, is the scenario ‘Do the best». In addition to the high cost associated with this, they sanctioned the procedure chosen as something insurmountable. The consequence is more serious. Why do we have to make an effort thinking if what we already do is “the best“ ? My only professional effort will focus, during my years of performance, to master the technique, without doubting its goodness and its alternatives. The surgery of the spine in the 90s, the treatment of pain and the pain units are paradigms of this. And what if it turns out that Fibromyalgia, Irritable bowel syndrome, migraine headaches, lower back pain, are a brain bug and not a pathology with damage that has a cure in 4 group sessions, with information only?.
Even worse than the above, is the scenario ‘Do the best». In addition to the high cost associated with this, they sanctioned the procedure chosen as something insurmountable. The consequence is more serious. Why do we have to make an effort thinking if what we already do is “the best“ ? My only professional effort will focus, during my years of performance, to master the technique, without doubting its goodness and its alternatives. The surgery of the spine in the 90s, the treatment of pain and the pain units are paradigms of this. And what if it turns out that Fibromyalgia, Irritable bowel syndrome, migraine headaches, lower back pain, are a brain bug and not a pathology with damage that has a cure in 4 group sessions, with information only?.
Will “Do it right” or “Do the best” never allow the organization to grow, learn or question the ground on which it stands, or the goodness of the ‘evidence of the moment ‘.
Organizations in which protocols rule – those who have decided that the blood pressure is taken 30 times a year to some patients, with the same impact that if they took it only once, or those in which algorithms become filters and forced step instead of information and expert knowledge help – these organizations are “zombie-like” and condemned to never produce amongst their ranks a Marshall or a Warren, or that if this was to occur, they will leave.
It will be an organization that will not have duodenal ulcers, because the population won’t have duodeno or gastric fundus, after so many gastrectomies, pyloroplasties and well done vagotomies.
Growth of the organization will only be possible with the scenario of «Do it better», or to put it more clearly, with the model focused exclusively in the goal of the achievement of «absence of peptic ulcers», allowing, provoking, stimulating and promoting that professionals think, try, rehearse, mistake hesitate, conclude, publish and emulate those that had succeeded in «more gastric health, with least-cost”
This requires, firstly, to remove every procedural obstacle (algorithm, Protocol) of the clinical Act, second, to measure 100% of expected epidemiological need, and, third, to return the information to the professionals so that they can think, try, experiment, fail and conclude.
And what to do now, in healthcare? Simply tell the professional that what you are going to measure is the reduction of the incidence of stroke, IAM and Arteriosclerosis, with this general budget and conclude with the authentic «Let’s see how you manage to achieve it!«.
Director!, let the professional be and respect the difficulty of his role! = Put pressure on him about purposes of health, give him a budget, measuring the final outcome and let him live, because his performance is complex for you to pretend to understand and master it without having worked in it. Director! – You don’t have to be dumb, nor should you seem to be one.
